高血鉀的原因幾乎都可以從低血鉀的機制反過來推,所以D/D比較不複雜(小麻居然連圖都沒有,哈哈),但是治療上面因為是Medical
emergency所以是重點唷。
1. 先排除pseudohyperkalemia
2. 區分出transcellular shift
3. 腎臟排出K的能力? 接著要評估的是腎臟排出K的能力,這部分可以分為三個層面來想
(忘記了請回頭看入門概述裡的 "正常生理對鉀離子濃度的調控"):
代表是tubule對aldosterone產生了抗性,以下是可能的原因
 高血鉀的原因幾乎都可以從低血鉀的機制反過來推,所以D/D比較不複雜(小麻居然連圖都沒有,哈哈),但是治療上面因為是Medical
emergency所以是重點唷。
高血鉀的原因幾乎都可以從低血鉀的機制反過來推,所以D/D比較不複雜(小麻居然連圖都沒有,哈哈),但是治療上面因為是Medical
emergency所以是重點唷。開始D/D
1. 先排除pseudohyperkalemia
- 含鉀的靜脈輸液、抽血時發生溶血、白血球血小板過多
2. 區分出transcellular shift
- 酸血症、insulin deficiency(DM)、大量細胞壞死(tumor lysis, 橫紋肌溶解, ischemic bowel, 溶血)、 hyperkalemic periodic paralysis、
- 藥物: β-blockers、毛地黃中毒、succinylcholine(機制:K+ efflux through AChRs-associated cation channels)
3. 腎臟排出K的能力? 接著要評估的是腎臟排出K的能力,這部分可以分為三個層面來想
(忘記了請回頭看入門概述裡的 "正常生理對鉀離子濃度的調控"):
- Distal Na delivery不夠?
- 別忘了ENaC吸收鈉是ROMK排出鉀的原動力
-
這裡抓的閾值Urinary Na < 25mmol/L
- Urinary Flow不夠?
-
別忘了Maxi-K/BK channel負責flow-dependent K
secretion,就是tubule分泌能力OK(TTKG>8),但是K總共分泌的量仍然不夠
(Urinary K < 40mmol/L),主要有兩個: - ECF不足(Aldosterone高,但尿腔的水也都被吸光了),或是
- Advanced kidney failure(eGFR<20,尿很少)
- Aldosterone不夠或是作用不好?
針對Aldosterone的功能,我們使用α-fludrocortisone(本院:Florinef)來做鑑別診斷。α-fludrocortisone的Relative mineralocorticoid activity是glucocorticoid activity的十倍,臨床上用來做Aldosterone的replacement
給α-fludrocortisone後TTKG有改善(>8)
代表本來是aldosterone製造不足的狀況,那我們得要看aldosterone的上游renin分泌的情況
高Renin:先天或後天primary hypoaldosteronism
- Primary adrenal insufficiency
- Isolated aldosterone deficiency:Loss-of-function mutations in aldosterone synthase
- Acquired adrenal insufficiency:Critical illness, amyloidosis, metastasis of carcinoma to the adrenal gland或Antiphospholipid syndrome造成bilateral adrenal hemorrhage
- Heparin/LMWH:↓adrenal aldosterone response to Angiotensin-II and hyperkalemia
- ACEi, ARB
- Ketoconazole:inhibit steroidgenesis
-
Adrenalitis in HIV patients(由CMV or tuberculosis造成)
低Renin:先天或後天secondary hypoaldosteronism
- 臨床常見後天因素:DM, old age, renal insufficiency, SLE, multiple myeloma, acute GN
- Interstitial nephritis:減少renin分泌
-
藥物:NSAID、COX-2 inhibitor、Aliskiren、β-blocker
給了α-fludrocortisone後TTKG卻沒改善(<8)
代表是tubule對aldosterone產生了抗性,以下是可能的原因
- Hyperkalemic distal RTA:SLE, sickle cell anemia, amyloidosis
- Renal transplant
- Pseudohypoaldosteronism (PHA)-I
- AD:Loss-of-function mutations of mineralocorticoid receptor
- AR:Loss-of-function mutations of ENaC
- Pseudohypoaldosteronism (PHA)-II,又稱Gordon syndrome
- Calcineurin inhibitors(Cyclosporine, Tacrolimus),背後的機轉有
- ↓COX-2 expression in the macula densa → Renin↓→ hyporeninemichypoaldosteronism
- Inhibit apical ROMK channels in the distal nephron
- Inhibit basolateral Na/K-ATPase
- 藥物: Amiloride, Spironolactone, Triamterene, Trimethoprim, Epterenone等等
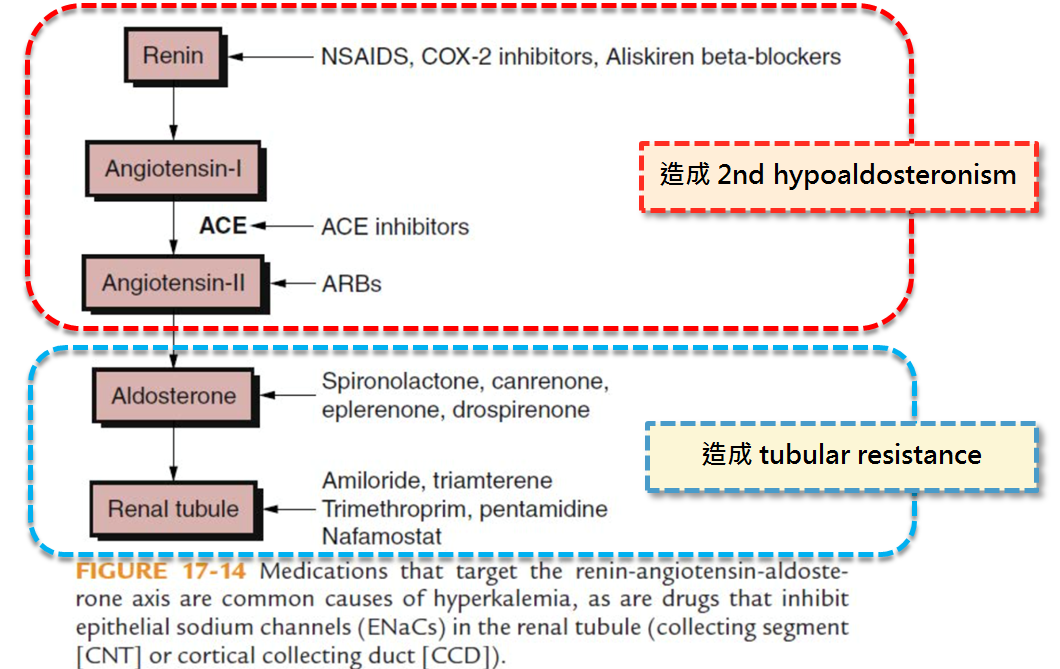
整理藥物對RAA system的影響
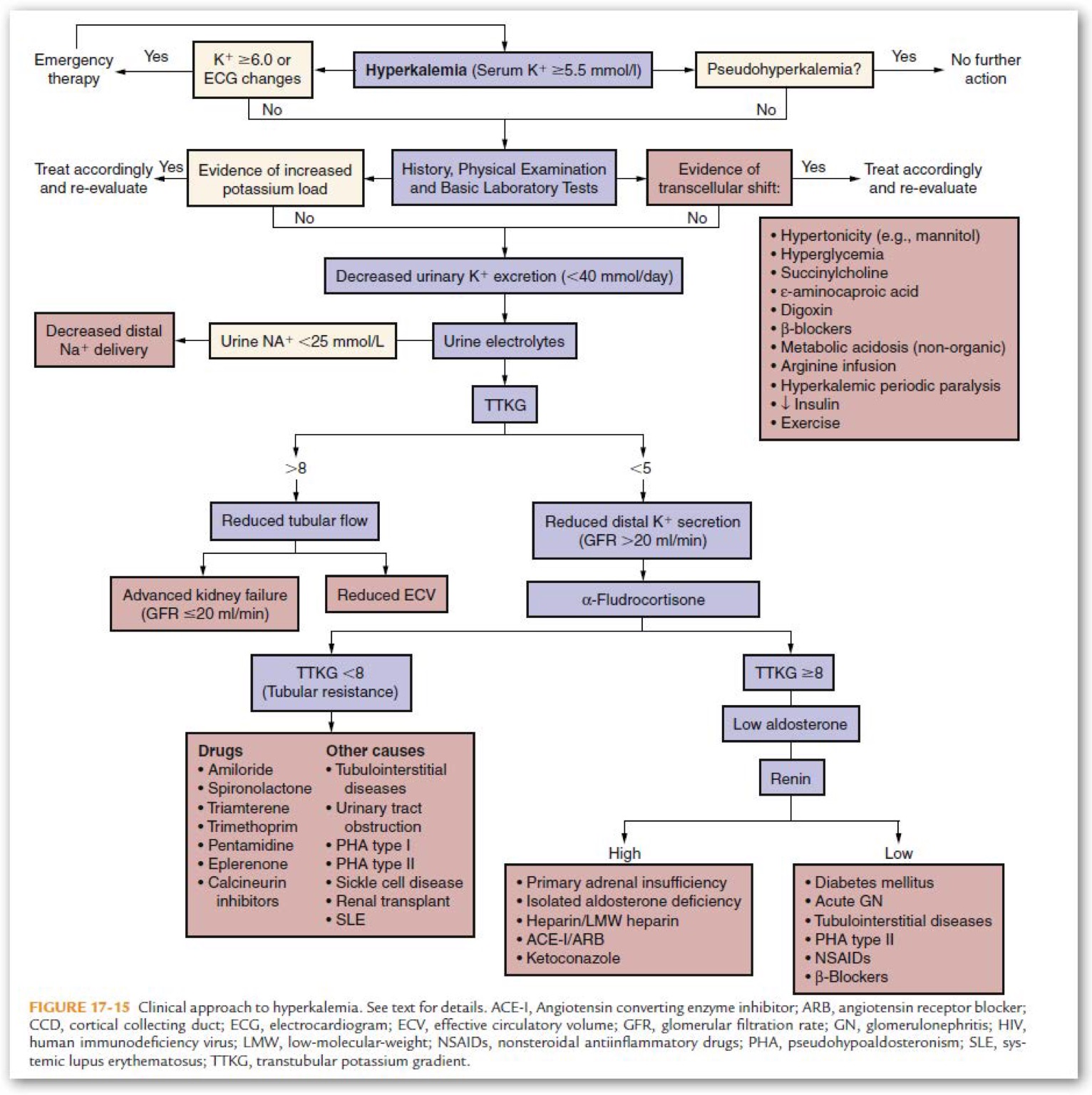
最後再來看一下完整的流程圖唷!
上一篇:[鈉與鉀]之14: 低血鉀 - 如何治療
下一篇:[鈉與鉀]之16: 高血鉀 - 你聽過Pseudohypoaldosteronism嗎?